

June 22, 2021
In the advertising industry, it seems the most powerful campaigns geared towards men specifically tend to target three primary insecurities: the lack of women in a man's life, a man's expanding waistline, and a man's empty wallet.
Yet there’s another insidious insecurity that plagues millions of men (and women) on a daily basis: their hairline.
Nothing scares many people more than the possibility of losing their precious head of hair.
Hair loss appears to be an ever-growing issue as you get older, and according to the American Hair Loss Association:
- 66% of men notice some degree of hair thinning by age 35, and this number goes up to 85% by the age of 50
- 40% of people experiencing hair loss are women, and almost 50% will experience some form of hair loss by age 50
As I was recently reading in a fashion magazine, hair has long been a primary indication of confidence for most men. When you consider that two-thirds of men see hair thinning by the age of thirty-five, and men’s hair restoration is a $1.5 billion industry, you began to understand how much confidence is attributed to a man’s hair. But why? In a Canadian survey conducted by researcher Rosemary Ricciardelli, men identified hair as being the primary link between their youth and attractiveness. Ricciardelli observed how men with a full head of hair—even the ones who weren’t particularly otherwise attractive—go out of their way to bring attention to their hair when meeting someone new. These full-haired men tended to be more relaxed and confident in demeanor when dealing with other individuals because they feel like they represent the standard for the ideal man.
Ricciardelli helped prove this theory by asking the participants to physically describe their ideal male figure. All of the participants described men who were clean-cut with a full head of hair. We’re unconsciously groomed (pun totally intended) and conditioned (ha!) to think that a healthy man has a full head of hair. But how does this psychologically affect the way men actually feel in their hair? Perhaps a full head of hair reassures them of their healthy biological standing. Maybe the loss of hair reminds men of their mortal vulnerability. Even men with gray hair prefer the color change over balding.
Interestingly beards also seem to matter, as facial hair is also a key part of men’s self-identification. In one study, men with facial hair were considered more aggressive than clean-shaven men. Both men and women found men with facial hair to be more masculine, with a higher social status, than men who were clean-shaven. More interestingly, men who are bald tend to accentuate their facial hair as compensation for balding. With the double whammy of baldness and facial hair, a man’s masculine appeal could be through the roof.
So, to continue on the topic of hair and beard health in men (and the former in women too) that I visited on my recent podcast with Dr. Cameron Chesnut, I decided to continue to explore the topic of hair optimization in today's article, written by my podcast guests (click here to listen) and friends Jay Campbell and Nick Andrews. This article and these two podcasts are part of a hair growth project that I kicked off back in early April that has been wildly popular—which is not surprising considering the statistics I quoted above.
Jay Campbell is a leading authority on full health optimization and more knowledgeable on the subject of therapeutic testosterone than practically any doctor you’ll ever meet. That’s on top of being a 4x international best-selling author and founder of the Jay Campbell Podcast.
Nick Andrews is the founder of Entera (which is what I use for my own hair these days) and one of the world’s top peptide product formulators. With over 20 years of first-hand experience in the pharmaceutical and cosmetic industries, his knowledge and foresight are unparalleled when it comes to therapeutic peptides and human biochemistry.
If you want to see me get into a deep-dive discussion with Jay and Nick on the subject of peptides, our podcast from April 2020 is still one of the best sources of information available online, and in the most recent episode, “The 2 Most Potent Hair Growth & Hair Loss Reversal Molecules Known To Humankind: C60 & GHK-Cu – A Big Hair Podcast With Auxano’s Jay Campbell & Nick Andrews.” Jay and Nick and I take a comprehensive look at a revolutionary, science-backed approach to treating hair loss.
You can also read some of Jay’s prior work on my website below:
- Testosterone Decoded, Shattering Testosterone Myths (& Everything You Need To Know About Testosterone Optimization Therapy).
- Is Metformin Really Dangerous, Little-Known Peptides For Muscle Gain & Fat Loss, Testosterone Replacement Therapy & Much More!
So buckle and get ready to have what you think you may know about DHT and hair loss challenged—and hopefully walk away with a new understanding of what you can do if you're one of the many people out there who are afflicted by hair loss insecurity.
What is DHT And How Does It Relate To Hair Loss?
Unfortunately, the first solution physicians and cosmeticians often present for hair loss and thinning hair is the wrong one: inhibiting the production of dihydrotestosterone (DHT).
This may seem like a very simple realization until you discover the entire multi-billion-dollar hair loss industry is predicated on the theory of DHT inhibition for stopping hair loss and initiating hair regrowth.
Today, you will be presented with a wealth of information that contradicts everything you may have seen or heard about hair loss. You may fight and resist the conclusions drawn in this article, but this information is being offered from a place of pure love. Not only is the DHT inhibition theory a failed rabbit hole for its intended goal, but you’ll also discover how it has caused untold hair loss to millions of men and women over the last 25 years.
To understand the flaws of the DHT inhibition theory, you first need to understand what DHT is and precisely why many people believe it is directly connected to hair loss.
DHT is primarily known as an androgen, which is a sex hormone directly derived from testosterone. It is responsible—alongside testosterone and other androgens—for male sex characteristics such as the growth of your reproductive organs, a deeper and lower voice, and increased muscle mass.
But DHT is also responsible for hair growth in every single part of your body. This includes the hair below your belt, the hair on your face, and the hair on your scalp.
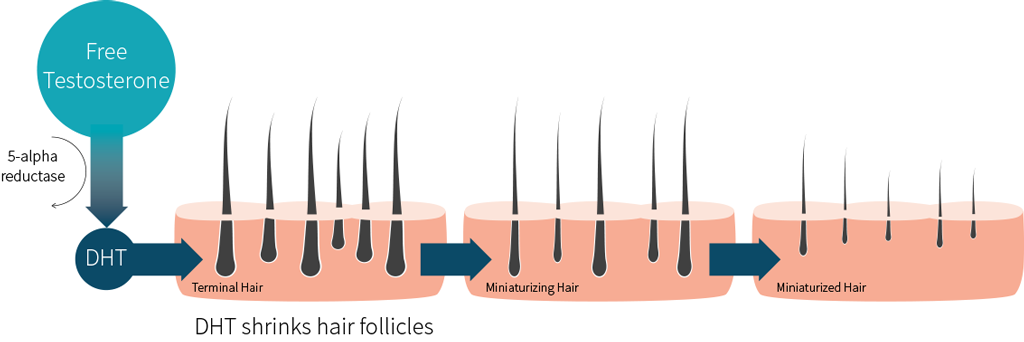
Let’s dive into the workings of the DHT inhibition theory using the image above.
DHT is produced from free testosterone in your body through an enzyme known as 5-alpha-reductase (5αR). And the theory postulates that the binding of DHT to the androgen receptors (ARs) on your hair follicles will lower hair production and consequently decrease the size of the hair follicles themselves. This is the basis behind blockbuster drugs such as Dutasteride and Propecia (a.k.a. Finasteride), which are clearly effective at lowering DHT production via the inhibition of 5αR activity.
One meta-analysis of clinical trials published in 2019 suggests Dutasteride is the superior DHT-inhibiting drug for treating male androgenetic alopecia, a hair loss condition caused by genetics, but this point is irrelevant. And while some doctors will mention that Dutasteride inhibits two separate types of 5αR and Finasteride only inhibits the type specifically found in hair follicles, it is also an irrelevant counterclaim.
What is relevant is the multiple holes in the DHT inhibition theory which simply do not stand up to the scrutiny of scientific evidence nor the blatantly contradictory results that are found in the real world.
The 5 Major Flaws Of The DHT Inhibition Theory For Reversing Hair Loss
When you take a deep dive into the medical literature and thoroughly evaluate the totality of evidence behind the DHT inhibition theory, the findings reveal that the correlation between DHT and hair loss is clearly weak.
An investigative look into the inner workings of DHT inhibition reveals multiple flaws…
1. The Body Hair Paradox
Despite rampant efforts to specifically block DHT production on your scalp, it is well-acknowledged in the medical literature that DHT is responsible for hair growth on every single part of your body. One study titled “Dihydrotestosterone Regulates Hair Growth Through the Wnt/β-Catenin Pathway in C57BL/6 Mice and InVitro Organ Culture” does a great job of summarizing this important principle:
“…androgens are essential for hair growth. Male pseudohermaphroditism patients show nearly no beard growth or [androgenetic alopecia] hair loss because of a lack of 5aR2, which suggests that DHT is necessary for beard growth.
Moreover, androgens regulate hair growth in both males and females… However, the mechanisms by which androgens have simultaneous but different effects on one organ, the [hair follicle], in different areas of the body in the same individual have not been well studied.”
Beard hair, pubic hair, chest hair, armpit hair…without androgens such as DHT that increase in production during puberty, growth of body hair—and thickening of said body hair—just doesn’t happen.
So what’s going on, then?
Why is it that DHT seems to work in the exact opposite manner when it comes to the hair on the top of your scalp?
In other words, why does DHT production lead to the loss of scapular hair, while leading to the growth of hair on other parts of the body?
It’s an interesting paradox to consider when you factor in how close the hair follicles on your face are to the ones on your scalp. Right?
2. Genetics Play A Role in Hair Loss
One small human study conducted in 2014 found an interesting discovery about male and female patients who suffer from androgenetic alopecia:
“…the most important factors would appear to be the genetically-determined sensitivity of the follicles to DHT and their different reactions to androgen concentration.”
We’ll emphasize the significance of genetics later on in this article, but it’s important to touch upon the conclusion of the study. Considering there are more than 250 genes associated with severe hair loss, something else is obviously at play when it comes to thinning hair.
3. Hair Loss in Females
While modern medicine confidently claims DHT is the culprit for male pattern hair loss, it is less assured when it comes to female pattern hair loss. In a 2012 study where androgen-deficient females with thinning hair were treated with testosterone for one year, the researchers were surprised to find that:
“Out of the 285 patients, 76 (27%) reported hair thinning prior to treatment; 48 of these patients (63%) reported hair regrowth on testosterone therapy (responders). Nonresponders (i.e. no reported hair regrowth on therapy) had significantly higher BMIs than responders (P = 0·05).
Baseline serum testosterone levels were significantly lower in women reporting hair loss prior to therapy than in those who did not (P = 0·0001). There was no significant difference in serum testosterone levels, measured 4 weeks after testosterone implantation, between responders and non-responders. No patient in this cohort reported scalp hair loss on testosterone therapy. A total of 262 women (92%) reported some increase in facial hair growth.”
This directly flies in the face of the DHT inhibition theory. If you recall the image presented earlier, increased testosterone would mean that more of it is available to be converted into DHT. (And if you paid close attention to the last sentence, some of those females even grew facial hair.)
We also have to consider that women can experience hair loss despite having significantly lower levels of testosterone (and DHT) on average than men. Furthermore, when you factor in “normal” testosterone levels relative to women, the DHT inhibition theory loses ground in explaining the causes of female pattern hair loss:
“Most women with the frontal-central pattern of hair loss have normal circulating androgens and do not present any other symptoms of hyperandrogenism, such as hirsutism or irregular periods/anovulation.
This type of hair loss has also been detected in women lacking an androgen receptor, with a deficiency of post-pubertal androgenization or the total absence of serum androgen. Dermatologists, therefore, use the phrase “female pattern hair loss” instead of androgenetic alopecia to avoid suggesting a role for androgen excess in this type of hair loss.”
We hope you’re starting to slowly see the DHT inhibition theory crumble, and you’ll start to see why correlating lower DHT levels with inhibited hair loss keeps us further away from understanding the root cause of hair loss.
4. Castration Doesn’t Do The Trick, Either
Thinking drastically, one might suggest the idea of castration in order to drastically reduce testosterone levels, thereby decreasing DHT production and inhibiting hair loss. We’ll later discuss why doing this is literal suicide for your hormonal health, but allow us to stay focused on the subject of hair loss.
In 1942, Dr. James Hamilton made the following observation about castrated men and hair growth:
“All men who failed to mature sexually had little or no dandruff and did not become bald. Common baldness occurs only in sexually mature individuals of families, the members of which tend to become bald. Androgenic therapy-induced baldness in eunuchoid and castrate members of such families only.
Cessation of treatment, as well as castration of normal men becoming bald, prevents further enlargement of bald areas, but apparently does not promote general regrowth of hair.”
The same observation was made by Dr. Hamilton in a 1960 study on young boys who were castrated before hair loss could even develop:
“A study of 21 adolescent and young adult males, before castration and for eight to eighteen years afterwards, showed that after orchiectomy there was no development of male pattern baldness (MPB) nor of any grossly recognizable denudation of the scalp. There was no expansion of bald areas in existence at the time of castration.
At the end of the study the eunuchs, compared with intact males of similar age, exhibited a significantly lower incidence of MPB (P = .01) and had no further loss of coarse hairs in the pattern that in most males results in recession of the frontal hairline (P <.01).”
To conclude Dr. Hamilton’s observations:
- Male pattern baldness was prevented in men who were castrated before the start of hair loss
- Hair loss (i.e. androgenetic alopecia) can be induced in castrated men who undergo testosterone injections
- Men who experienced hair loss first and then got castrated were at a standstill, where balding neither progressed further nor reversed
Put another way, Dr. Hamilton’s work was the basis on which people falsely believed testosterone—and consequently DHT production—was directly correlated with hair loss.
To make things even more interesting, there was a little-known study published in 1974 involving male pseudohermaphrodites who lived in rural villages within the Dominican Republic. Specifically, these individuals suffered from a rare deficiency in the 5αR enzyme. (Remember: 5αR is the enzyme responsible for converting testosterone into DHT. No enzyme, no DHT production.) If you don’t immediately understand the implications of being a pseudohermaphrodite, the study explains the phenomenon briefly:
“At birth, the subjects have a marked bifid scrotum that appears labia-like. There is a clitoris-like phallus and a urogenital sinus with a blind vaginal pouch. The testes are in the abdomen, inguinal canal, or scrotum.
However, during puberty, under the influence of normal plasma testosterone levels, definite virilization occurs. The voice deepens, and affected subjects develop muscular habits. There Is substantial growth of the phallus and the scrotum becomes rugged and hyperpigmented. In most subjects, the testes descend into the scrotum if they have not already done so.”
But what’s even more fascinating is none of them suffered from male pattern hair loss… yet it’s surprising to see these same 5αR-deficient people have little to no hair everywhere else on the body.
By now, it should be clear that your testosterone levels are irrelevant to hair loss:
“Both low and high levels of testosterone can result in hair loss. We need to understand that those with low testosterone levels may in fact have the same amount of DHT that contributes to hair loss. It has been shown that men with male pattern baldness have low testosterone levels with average DHT levels in their body.”
Even then, it is unclear whether DHT levels stay the same or decrease as you age. Yet given that it's a fact that your body’s natural production of testosterone decreases with age, shouldn’t DHT production also fall? And shouldn’t hair loss consequently slow down over time as a result?
5. The “Gravity Theory” Of Hair Loss
This final point before addressing other major holes in the DHT inhibition theory may seem bizarre in nature. Everything you’ve read up to this point may lead you to believe hair loss is entirely related to genetic susceptibility. Regardless of your DHT levels or those of other androgens, some people are simply fated to experience hair loss.
There may be some truth to this, but it’s not the entire picture.
At the very least, it can be said with complete confidence that DHT does not directly cause hair loss. So something else has to be at play here.
Dr. Emin Tuncay Ustuner, a plastic surgeon in Ankara, Turkey, came up with the “gravity theory” in 2013 to explain the paradoxical observations seen in men undergoing hair loss despite clear differences in their hormonal profiles. His published paper on the topic asks the exact same questions we’ve put forward in this article, and explains how genetics can contribute to androgenic alopecia… but not in the way you think.
ScienceDaily has a good summary of the gravity theory, posted here in its entirety as the theory cannot be explained any more succinctly:
“In youth, the scalp has sufficient fat tissue under the skin, and it is ‘capable of keeping itself well-hydrated,’ buffering the pressure on hair follicles. But with aging, the skin and underlying (subcutaneous) fat become thinner, and the pressure on the hair follicles increases. Testosterone contributes to thinning of the subcutaneous fat.
As the cushion decreases, the hair follicle must strive against higher pressure, requiring more testosterone to achieve normal growth. This “local demand” leads to a buildup of DHT levels in the scalp, but not in the bloodstream. Rising DHT levels cause further erosion of the subcutaneous fat — creating a vicious circle.
The hair growth cycle accelerates in response to DHT, but it's not enough to overcome the increased pressure. Over time, the hair follicle becomes smaller and smaller, resulting in progressively increasing hair loss.”
(If you want to read the full technical paper that goes into much further detail, go here.)
Dr. Ustuner goes as far as to suggest that the shape of your head, which is entirely genetic, explains why DHT makes hair follicles thinner on your head and thicker on every other part of your body. And hence why DHT seems to promote hair growth everywhere except for your scalp.
This theory explains why hair loss tends to be concentrated on a particular region of your head called the galea aponeurotica:
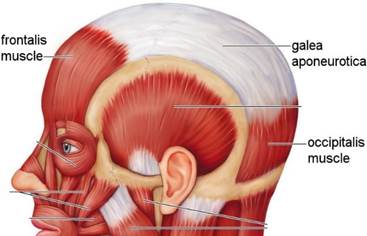
Which just so happens to be where male pattern baldness takes place:

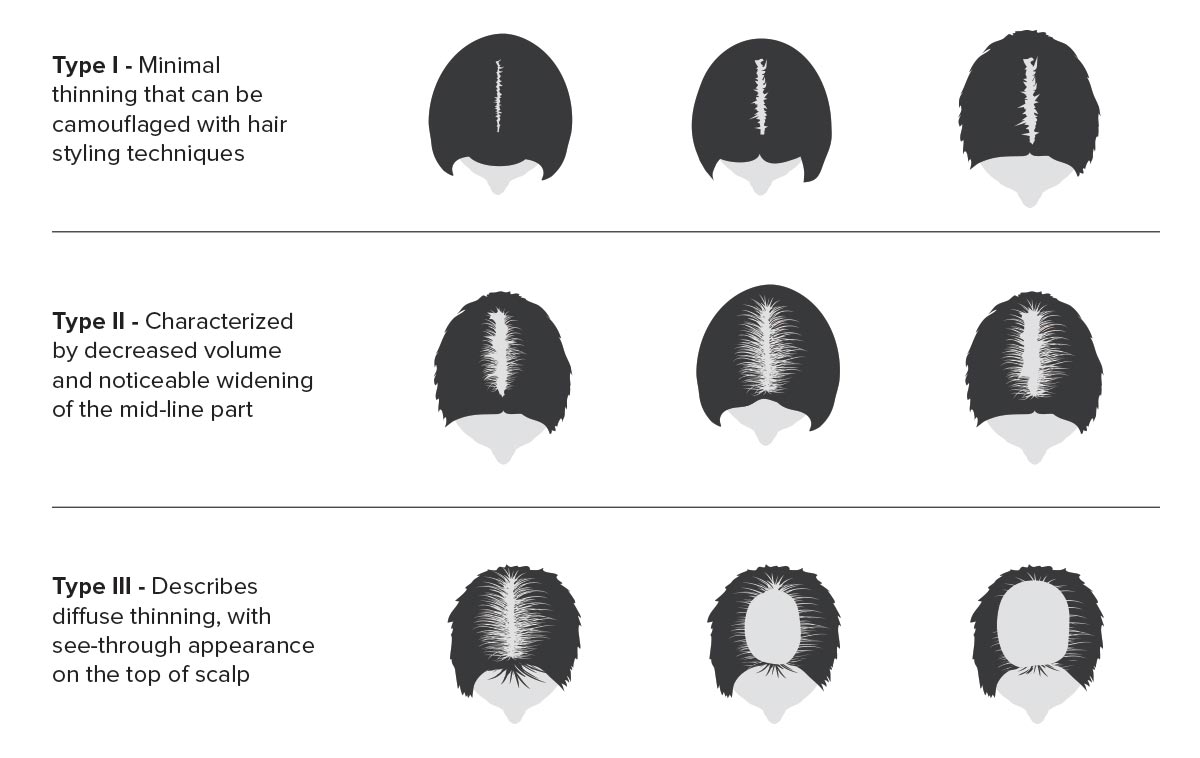
It looks a little different for females due to their unique head shape, but the same observation is noted:
Somehow, hair follicles behave and react differently when they are located in the galea aponeurotica versus other parts of the scalp.
Are there perhaps multiple biological environments within the scalp?
One possible explanation for the differentiation could be the lack of blood flow to the galea aponeurotica, meaning this area seems to receive less oxygen and nutrients compared to different regions of the scalp. The only evidence supporting this is a study involving 40 men suffering from hair loss who received Botox injections into their scalp:
“…no adverse effects were reported. The treatment response rate was 75 percent. Mean hair counts for the entire group showed a statistically significant (p < 0.0001) increase of 18 percent between baseline and week 48, similar to the results reported with Propecia. Hair regrowth was objectively visible in some subjects.”
Furthermore, the explanation for these results seems to line up with the ideas put forth by the gravity theory:
“Botox ‘loosens' the scalp, reducing pressure on the perforating vasculature, thereby increasing blood flow and oxygen concentration. The enzymatic conversion of testosterone to dihydrotestosterone is oxygen-dependent. In low-oxygen environments, the conversion of testosterone to dihydrotestosterone is favored; whereas in high-oxygen environments, more testosterone is converted to estradiol. Blood flow may therefore be a primary determinant in follicular health.”
Another study examining the use of scalp massages seems to support the idea of reduced blood flow, in which healthy Japanese males used an at-home device to treat themselves:
“Nine healthy men received 4 minutes of standardized scalp massage per day for 24 weeks using a scalp massage device. Total hair number, hair thickness, and hair growth rate were evaluated.
Standardized scalp massage resulted in increased hair thickness 24 weeks after initiation of massage (0.085 ± 0.003 mm vs 0.092 ± 0.001 mm).
“Stretching forces result in changes in gene expression in human dermal papilla cells. Standardized scalp massage is a way to transmit mechanical stress to human dermal papilla cells in subcutaneous tissue. Hair thickness was shown to increase with standardized scalp massage.”
In other words…elevated DHT is not a direct causal effect of hair loss, but a downstream secondary effect of some primary mechanism taking place.
But before addressing what that primary mechanism of hair loss actually is, let’s talk about why DHT inhibition is destructive for your hormonal health and overall well-being.
9 Negative Health Effects of DHT Inhibition
Have you ever considered that lowering your body’s DHT levels, even if using a cream applied only to your scalp, has possible downstream hormonal consequences?
If not, there's bad news for you: it does.
And when you read what lies in your future upon DHT inhibition, you’re likely to think twice before picking up a script from your doctor.
1. Sexual Health
One meta-analysis of Finasteride and Dutasteride found the drugs negatively impact a man’s “performance” in several ways:
Lowered Libido
“…most of the studies reported that inhibition of 5α-R contributes to reduction or loss of libido. Finasteride and dutasteride produced decrease in sex drive at week 26 and 52 of drug treatment. Drug-related reduction in libido occurred in 4.2% and 1.8% of patients in the dutasteride and placebo groups, respectively. In a 2-year follow up of patients in the CombAT trial, approximately 2.8% of the dutasteride group had decreased libido and 1.3% of the group experienced complete loss of libido.
Some patients have reported persistent loss of libido after discontinuation of the drug. Although these numbers may appear low or insignificant, their impact on the overall quality of life is not easily measured.”
Erectile Dysfunction
“ED is consistently observed in double-blind, randomized, placebo-controlled trials…Approximately 6–8% of patients reported ED in several trials. In an observational cohort of 14,772 taking finasteride, ED was the most common adverse event, leading to withdrawal (143 patients).
The AUA clinical practice guideline reported erectile problems in 8% and 4% of patients taking finasteride and placebo, respectively.”
Reduced Ejaculatory Function
“…ejaculatory function is adversely affected in 5α-RIs trials. Finasteride and dutasteride treatment resulted in a decrease in ejaculatory function at week 26 and 52, as determined by the sexual function inventory. The CombAT study observed 0.6% retrograde ejaculations, 0.5% ejaculation failure, and 0.3% semen volume decrease in patients.
The AUA clinical practice guideline's review of 5α-RI trials suggested that 4% and 1% of patients taking finasteride and placebo had sexual ejaculation dysfunction, respectively, suggesting that the results pertaining to ejaculatory function are mixed and additional data are needed to ascertain the drug impact on ejaculation.”
Frankly, decades of data on Finasteride exist which suggest there are an awful lot of men whose sexual health has been ruined by this drug:
“Starting in the 1990s, independent studies described sexual adverse events such as erectile dysfunction (ED), decreased ejaculate volume, and decreased libido in young men who used finasteride against MPHL. In some men, these side effects persisted for months or even years after finasteride discontinuation. Additionally, several case reports described patients on low-dose finasteride with impaired spermatogenesis, which was reversed after drug cessation.”
2. Higher Risk of Osteoporosis (i.e. Bone Tissue Degeneration)
Another meta-analysis regarding the adverse events associated with 5αR-inhibiting drugs picked up an interesting observation about bone health:
“A recent study on the effects of 5α-Rs inhibitor on bone in men treated for BPH [benign prostatic hyperplasia] in the Taiwanese National Health Insurance Research Database (NHIRD) which comprised of 1352 men with diagnosis of osteoporosis and 5387 men as control cases without osteoporosis diagnosis.
In this population, nested control study the authors noted that a 1.52-fold increase in osteoporosis diagnosis among patients with BPH treated with finasteride (95 % CI, 1.01–2.30) compared with controls. They also noted that higher doses of finasteride were associated with higher osteoporosis diagnosis risk (OR=1.68; 95 % CI, 1.01–2.81), compared to controls.”
Something worth thinking about if you desire mobility and the freedom to move your body as you get older!
3. Fat Accumulation
Much like testosterone, lower levels of DHT are significantly associated with greater levels of visceral adipose tissue:
“Paired omental and subcutaneous adipose tissue samples were surgically obtained from 60 women (age, 47±5 years; body mass index, 26±5 kg/m2) undergoing gynecological surgery. Body composition and fat distribution were measured by dual-energy X-ray absorptiometry and computed tomography, respectively.
Significant negative associations were found between plasma dihydrotestosterone (DHT) levels and total adiposity (body mass index, r=-0.35, p<0.05; fat mass, r=-0.31, p<0.05) as well as computed tomography assessments of abdominal adiposity (r=-0.30, p<0.05 and r=-0.44, p<0.005 for subcutaneous and visceral adipose tissue area, respectively). The association between DHT levels and visceral adipose tissue area was independent of total body fat mass.”
And in older men suffering from androgen deficiency, using DHT helped them change their body composition for the better:
“This study evaluated the efficacy and safety of 3 months treatment with transdermal dihydrotestosterone gel on muscle strength, mobility, and quality of life in ambulant, community-dwelling men aged 60 yr or older. Eligible men (plasma T ≤15 nmol/liter) were randomized to undergo daily dermal application of 70 mg dihydrotestosterone gel (n = 18) or vehicle (n = 19) and were studied before, monthly during, and 1 month after treatment.
…dihydrotestosterone had significant effects on circulating hormones (increased dihydrotestosterone; decreased total and free testosterone, LH, and FSH; unchanged SHBG and estradiol), lipid profiles (decreased total and low-density lipoprotein cholesterols; unchanged high-density lipoprotein cholesterol and triglycerides), hematopoiesis (increased hemoglobin, hematocrit, and red cell counts), and body composition (decreased skinfold thickness and fat mass; unchanged lean mass and waist to hip ratio).”
4. Increased Risk of Gynecomastia
Speaking of being unhappy with your body… what would happen to a man’s self-esteem if he developed “man boobs” (i.e. gynocomastia)? It would crush him and he would feel uncomfortable taking his shirt off in public. And in Jay’s personal experience, dealing with gyno can be very painful.
This is why it is strongly advised to stay away from drugs like Finasteride and Dutasteride:
“…gynecomastia is among the adverse side effects of 5 aRIs experienced by patients placed on this therapy. Gynecomastia had been observed in 214 men receiving finasteride therapy according to reports to the U.S. Food and Drug Administration from 1992 to 1995.
In the Prostate Cancer Prevention Trial (PCPT), approximately 426 of 9,423 subjects (4.5%) in the Finasteride arm had gynecomastia compared with 261 of 9,457 subjects (2.8%) in the placebo arm. In men taking finasteride alone or with doxazosin, 4 out of 1,554 developed breast cancer, a rate approximately 200 times that of the general population. Inhibition of 5a-DHT synthesis by 5a-RIs may shift metabolism of T toward estradiol (E2) and alter the estrogen to androgen ratio, thus increasing the risk of gynecomastia and male breast cancer.”
5. Failure To Benefit From Testosterone Optimization Therapy
If you already read Jay’s guest article on therapeutic testosterone, you already know about the life-changing benefits it can offer you. You also know that it is criminal for know-nothing doctors to artificially suppress a man’s estrogen levels in hopes of keeping them at an “optimal” range of estrogen:
“Testosterone must aromatize into estradiol (estrogen) to confer protection to the biological system. Estradiol is a pleiotropic hormone that has instrumental influence over numerous critical functions related to the cardiac and vascular system, bone and mineral metabolism, cognition, memory, mood, balance, age-related neurodegenerative disorders and lipolysis(burning) of fat. When a doctor places a patient on an AI to attempt to resolve “estrogen-related symptoms” or to keep the patient in a perceived ‘narrow” or “optimal lowered range” of estrogen, a whole host of negative endocrine system reactions can and often does occur.”
As it turns out, just as testosterone must be allowed to aromatize into estradiol (E2) to confer estrogen’s protective effects to multiple biological systems, testosterone must be allowed to convert to DHT in order for DHT to exert its needed important biological effects:
“Almost 10% of the testosterone produced by an adult each day is converted to dihydrotestosterone, by the testes and prostate (in men), the ovaries (in women), the skin and other parts of the body it is thought that the increased dihydrotestosterone production may be responsible for the start of puberty in boys, causing development of the genitals (penis, testes and scrotum) and growth of pubic and body hair. This hormone also causes the prostate to grow and is thought to combine with testosterone causing the expression of male sexual behavior. Dihydrotestosterone is many times more potent than testosterone, and many of the effects that testosterone has in the body only happen after it is converted to dihydrotestosterone.”
6. Higher Rates of Depression
Although this side effect appears to be debated hotly by scientists, there is some evidence suggesting 5αR inhibitors can increase the frequency and severity of depressive symptoms:
“An inverse relationship between levels of AP [allopregnanolone] and depression has been demonstrated in male patients with depression. Preclinical studies have suggested that reduction in AP levels by [5α-R inhibitors] may contribute to depressive symptoms. Increased depressive symptoms are thought to be linked to finasteride treatment. A statistically significant correlation was observed between use of finasteride and depressive symptoms.
Persistent side effects have been noted even after discontinuation of finasteride treatment from 3 months to 11 years, suggesting that the adverse effects of finasteride may be permanent.”
And if all of this wasn’t enough to convince you to explore better avenues for treating hair loss, maybe this one will…
7. Post-Finasteride Syndrome (PFS)
Yes, there is an entire foundation devoted solely to the treatment of PFS:
“Post-finasteride syndrome (PFS) describes persistent sexual, neurological, physical and mental adverse reactions in patients who have taken finasteride, a 5-alpha reductase type II enzyme inhibitor used to treat hair loss (under the brand name Propecia or generics) or enlarged prostate (Proscar or generics).
Unfortunately, PFS is a condition with no known cure and few, if any, effective treatments. As an increasing number of men report their persistent side effects to health and regulatory agencies worldwide, medical and scientific communities are only beginning to realize the scope of the problem.”
There are so many potential side effects of this drug that you may never know existed, including:
- Fatigue: Chronic fatigue, listlessness
- Self-Harm: Attempted/completed suicide
- Sleep: Insomnia, obstructive sleep apnea
- Memory: Severe memory/recall impairment
- Cognition: Slowed thought processes, impaired problem solving
- Skin: Chronically dry, thinning of the skin
Want to know what else is so devastating about Finasteride and Dutasteride?…
8. Lifelong Dependency on DHT-Inhibitors
Get ready for an entire lifetime of dependence on the pharmaceutical industry.
Much like the majority of Big Pharma medications…once you are on a DHT-inhibiting drug for hair loss, you are glued to it forever:
“Once you stop taking finasteride, the dose of the medication that’s active in your body will slowly decline until it’s completely excreted over the course of several days.
…If you’re genetically prone to male pattern baldness, this can mean that the DHT will once again start to affect your hair follicles, resulting in thinning of the hair on your scalp, hairline recession, and other male pattern baldness effects.
“In short, if you stop taking finasteride daily, you’ll lose the hair you’ve gained in about one year. Finasteride isn’t a lifetime cure — instead, it’s a treatment that you need to keep taking if you want to continue to stop hair loss.”
Stopping Finasteride use means no more 5αR inhibition. Stopping 5αR inhibition means DHT affects your hair follicles again and hair loss resumes. Sadly, other hair loss agents (as you’ll later find out) aren’t so hot either.
9. Major Safety Issues in Clinical Trials
We’re not saying the 5αR-inhibiting drugs don’t “work.” In the literal sense, they do exactly what they say and lower your body’s DHT levels significantly. And certainly, there is some degree of hair loss reversal coupled with hair growth.
But as you have already seen, the side effects are significant, and inhibiting DHT is just as bad of an idea as inhibiting estrogen.
The majority of clinicians still promote these drugs as safe and effective, claiming the side effects are extremely rare in nature. However, there were some major issues with the studies these same clinicians will commonly cite when discussing the safety of 5αR-inhibiting drugs:
“Of 34 clinical trials, none had adequate safety reporting, 19 were partially adequate, 12 were inadequate, and 3 reported no adverse events…Available toxicity information from clinical trials of finasteride in men with [androgenic alopecia] is very limited, is of poor quality, and seems to be systematically biased.”
You now have a serious incentive to refuse Big Pharma’s recommendations and go elsewhere for effective hair loss treatments.
Multiple Factors Are Simultaneously Involved In Hair Loss
If DHT is only one piece of the puzzle, surely there are other factors in hair loss that must be taken into account.
Indeed there are…
…and while Jay has also discussed them at length on here, they are worthy of repeating.
- Medications such as SSRIs, blood pressure drugs, and certain antibiotics have hair loss as a possible side effect.
- Your genetic makeup, specifically the sensitivity of the androgen receptors in your hair follicles that interact with DHT (i.e higher sensitivity = greater hair loss).
- Chronic stress levels leading to telogen effluvium, a condition in which hair is continually shed.
- Poor lifestyle habits such as smoking, alcohol, pre-existing medical conditions, and god-awful nutrition.
- Environmental contaminants such as endocrine-disrupting chemicals (EDC’s) are also associated with hormonal hair loss in women.
But there are some other unexplored root causes including:
- Cellular dysfunction of the hair follicle cells themselves, which can also lead to age-associated hair loss through cellular senescence.
- Restriction of blood flow to the impacted area of the scalp (this has already been mentioned but many hair loss experts understate its significance).
- Emerging new evidence (here, here, and here) suggests reversing mitochondrial dysfunction (i.e. restoring the health of your mitochttps://www.ncbi.nlm.nih.gov/pmc/articles/PMC7432488/hondria) may help reverse hair loss.
The solution seems simple, then: Restore your follicular health via multiple mechanisms, ranging from enhancing angiogenesis (synthesis of new blood cells) in your scalp’s dermis to improving mitochondrial function, enhancing your body’s cellular energy metabolism, and cleaning up your lifestyle.
But there’s just one more root cause worth talking about…
Chronic Inflammation In the Scalp
Believe it or not, micro inflammations of the scalp can greatly contribute to hair loss and hair thinning. Not only is the skin surrounding your hair follicles inflamed, but your hair roots are also weaker in strength:
“Recently, particular focus has been given to hair cortisol concentration (HCC) as a promising diagnostic instrument in clinical practice. Hair cortisol concentration was also reported to have an impact on correct hair growth. The presence of cortisol in high levels is strictly connected with a reduction in the synthesis and premature degradation of hyaluronans and proteoglycans—important modulators of hair follicle function. However, low cortisol levels can actually bring positive effects on hair growth by slowing down the degradation of these two skin components.”
Additionally, part of the body’s natural inflammatory response when wounds are being healed involves increasing production of DHT:
“(1) chronic scalp tension transmitted from the galea aponeurotica induces an inflammatory response in androgenic alopecia-prone tissues;
(2) dihydrotestosterone increases in androgenic alopecia-prone tissues as part of this inflammatory response; and
(3) dihydrotestosterone does not directly miniaturize hair follicles.
Rather, dihydrotestosterone is a co-mediator of tissue dermal sheath thickening, perifollicular fibrosis, and calcification – three chronic, progressive conditions concomitant with androgenic alopecia progression.”
In simpler terms, the inflammation is induced by chronic contraction of the muscles in your scalp connected to the galea aponeurotica. The inflammatory response is the primary event, while increased DHT production is the secondary result.
So when you block DHT, you’re reducing the inflammatory response while failing to treat the inflammation as the root cause.
This is how – using modern medicine's preferred form of “stopping” hair loss – people mess up their hormonal health while failing to fix their hair loss, thus setting themselves up for other unwanted and unnecessary side effects.
Other Traditional At-Home Hair Loss Treatments Are Ineffective
Hopefully, by now you are convinced that drugs that lower DHT production is not the answer, but it also can't be said that the traditional alternatives are much better.
Jay has written about them extensively, but here’s the high-level summary:
Minoxidil (Rogaine): Works through increasing blood flow to the hair follicles and promotes hair follicle growth, but like Finasteride and Dutasteride you’re chained to it for life. It also fails in roughly 39% of people who take it and you need the prescription-strength variant. That’s on top of accepted use side effects such as fatigue, red itchy scalp, nausea, and vomiting.
Natural over-the-counter supplements: Significant lack of evidence demonstrating long-term hair loss reversal and hair growth, and are completely unregulated.
Hair transplant surgeries: Extremely expensive (several thousands of dollars for one session), the transplanted hair thins over time, you may need multiple transplants (even then there’s a limit before you permanently damage your scalp tissue), and there are numerous things that can go wrong during the surgery. Plus it is often obvious to people you’ve had “work” done.
Summary
So there you have it. In summary, DHT is an androgen produced from free testosterone in your body through an enzyme known as 5-alpha-reductase (5αR).
The DHT inhibition theory posits that inhibiting DHT binding to receptors in your hair follicles should increase hair production.
This is the prevailing wisdom in regards to hair loss reversal. Popular drugs such as Finasteride and Dutasteride work on the basis of this theory. However, the following considerations—when taken together—unequivocally prove that the DHT inhibition theory is flawed:
- DHT is crucial for hair growth in every single part of your body. It's illogical that the scalp would respond differently to DHT than other hair follicles.
- Genetics also play a large role in determining how “sensitive” receptors in your hair follicles are to DHT binding (i.e. increased sensitivity = more binding).
- Females treated with testosterone, the precursor to DHT, experience hair growth on their heads and their faces. They also have lower levels of DHT in their bodies than men, yet they still experience hair loss.
- Castrated men (i.e. extremely low levels of testosterone and DHT in their bodies) who do not experience scapular hair loss can have it induced with testosterone injections, yet experience little to no hair growth in other parts of their body.
- Hair loss happens regardless of testosterone levels being high or low—if testosterone levels and DHT levels decrease with age, then why does hair loss accelerate?
Inhibiting DHT in an attempt to reverse hair loss is not just ineffective—it can be disastrous to your health. The negative side effects of DHT inhibition include:
- Lowered libido
- Erectile dysfunction
- Reduced ejaculatory function
- Higher risk of bone degradation (osteoporosis)
- Increased visceral fat accumulation
- Greater chance of developing gynecomastia
- Lower success rate with using therapeutic testosterone
- Higher rates of depression
- Post-Finasteride Syndrome (“persistent sexual, neurological, physical and mental adverse reactions, with no known cure and few treatments, if any)
- A lifelong dependency on using DHT-inhibiting drugs (you stop using them and the hair loss resumes and often accelerates)
- Many of the clinical trials vouching for the efficacy of DHT-inhibiting drugs often suffer from a lack of inadequate safety reporting
What the evidence and research do clearly show is that there are multiple factors simultaneously involved in hair loss. DHT is part of the equation, but not in the way that is currently presumed. For example, your head shape, which is entirely genetic, may explain why DHT promotes hair loss exclusively on the scalp (due to the fat cushion on your scalp becoming thinner with age, increasing pressure on hair follicles, and leading to the opposite expected effect). What is known is that elevated DHT is not a direct causal effect of hair loss, but a downstream secondary effect of some primary mechanism taking place.
The elements that are involved and need to be considered when addressing hair loss include:
- Certain kinds of medications
- Your genetic makeup
- Chronic stress levels
- Epigenetic factors leading to systemic inflammation (poor sleep, nutrition, lack of exercise, smoking, excess consumption of sugar and alcohol)
- Endocrine-disrupting chemicals (EDC’s) in the environment
- Restriction of blood flow to the scalp leading to micro-inflammation in the follicles
- Mitochondrial dysfunction
- Cellular senescence
You may be thinking: all of this is well and good, but if DHT inhibition isn't the answer, what can I do to get that full head of hair (back)? In next week's article, Jay and Nick will take a comprehensive look at what works based on the latest scientific research. In the meantime, you may also enjoy this recent podcast Ben recorded with a beauty and anti-aging physician named Cameron Chesnut, in which we explore several of these issues in an audio.
I'd love to know if this article has changed your thinking about hair loss. Have you tried DHT inhibition to reverse hair loss? Do you have any hair growth or beard care tips? Leave your questions, comments, and thoughts below. Jay, Nick, or I will respond!












Interesting read… i just have a question… why were those kids being castrated in the 1960 study?? Who in their minds would castrate children? Sounds like child abuse -_-
(And as i write this, today’s modern day irony hit me… but there wasn’t a transgender fad going on in those days..) … i’m am genuinely curious trying to understand what was going at that time in history and trying to understand humans, and why they would subject themselves and others to such sadistic measures…
good grief. there are good humans and bad humans. those humans are obviously some of the worst. there is nothing to understand. there is no deep meaning. people are broken. people need to be put down. you know how many animals are put to slaughter every year? 800,000,000 cows, 30,000,000,000 chickens. the world is ugly and violent.
Hello,
An entertaining read, thank you for taking the time to research it and write it out.
However, if anything, this entire article is more of an advertisement for how effective 5AR inhibitors actually are at reducing hair loss… and also how ineffective all other treatments are.
Yes, you did a fantastic job of going through recorded side effects, and they absolutely do exist. However, when you weigh the level of effectiveness of limiting hair loss with the slim risk (1% in most studies) of an adverse side effect, it’s no wonder Finasteride in particular is prescribed by doctors as frequently as it is.
As a result, this article comes across as biased and even almost clutching at straws at times with the conclusions and ideas presented. For example:
– Hair on your scalp is an entirely different type of hair follicle to facial and pubic hair, yet you made zero reference to this and instead called them not acting the same “illogical”.
Moral of the story for those on the fence:
– Research 5AR Inhibition extremely well, be aware of the side effects so you can spot them.
– Stop the medication if you are one of the unlikely 1/100 people who experience an adverse side effect.
Hello,
An entertaining read, thank you for taking the time to research it and write it out.
However, if anything, this entire article is more of an advertisement for how effective 5AR inhibitors actually are at reducing hair loss… and also how ineffective all the other treatments are.
Yes, you did a fantastic job and going through recorded side effects, and they absolutely do exist. However, when you weight the level of effectiveness of limiting hair loss with the slim risk (1% in most studies) of an adverse side effect, its no wonder Finasteride in particular is prescribed by doctors as frequently as it is.
Moral of the story for those on the fence:
– Research 5AR Inhibition extremely well, be aware of the side effects so you can spot themabsolutely
Be mindful of:
1) Effective it is at limiting hair loss and
2) Stop the medication if you are one of the the unlikely 1/100 people who experience an adverse side effect.
Hi Ben Thanks for the informative article. I’m 61yrs old, have thing hair with shorter and thinner hair follicles towards the posterior galea aponeurotica vs longer follicles mid and anterior galea aponeurotica. Do you know of any studies mentioning this and or any correlation presented as part of the Gravity Theory? Has anyone else notice this? I have not as of yet tried any hair restoration products, and was happy to find this recent article. I see my instincts to skipping using the mainstream products seems justified. Looking forward to part 2. I’m a novice biohacker always looking for cutting edge science backed information. By the way, thanks for writing Boundless. There’s a wealth of knowledge in it.
Thank you for the great article! As a woman who has noticed her hair thinning over the last decade, this information is great and confirms my general gut feeling…switching to all natural shampoo, getting rid of the constant ponytail, focusing on lifestyle and less stress ( hard to do with two kids under 5), and also gave me some great ideas to try next :)! Keep the great information coming!!!
There was so much in this I’m still processing. But I tossed out my finasteride halfway through reading this. I’ve noticed SO many side effects since starting it a year ago and no where near the level of regrowth I’d like. Will be impatiently waiting for the follow up to this.
Some time ago I was using SAW PALMETTO. It decreases DHT.
My libidos was going down and down. Never more.
Eduardo, I’m taking a pill that has Biotin and Saw Palmetto. Gonna throw that bottle out now. Glad you said something about it.
It’s great to know that there may be other options for a man besides the sharp dht reduction and choosing between hair or your manhood. I’ve tried many things with mixed results. Recently, stacking a red light hair helmet, scalp massage, with biotin, he shou wu and black seed oil has been relatively effective. I still haven’t found a great topical so keen to explore the ones mentioned. Hormonal balance seems very important as I noticed when taking too much creatine and dhea, my shedding increased so I backed off. Thoughts on these? Thanks for the insightful article! 43 yr old biohacker.
I am a Hair Educator and in all honesty, having coached over 100 students – the more I teach, the more I learn and Epigenetics is huge when it comes to determining the actual root cause of Hair Loss.Treating the root cause of the systemic inflammatory reactions is the key in stopping exacerbated hair loss by introducing sustainable lifestyle changes, effective dose of supplements, right products based on your hair profile, building a hair care routine, DIYs and of course internalising positive affirmations every time we take care of our selves.
Please feel free to reach out to me whoever comes across my comment and I d be so happy to guide you through to realise each and every one of us has the power to have the hair and health we deserve because we only deserve the Best.
Instagram : @cagetheage
Agree Manissha. We create our reality (in this simulation) through our thoughts, words and actions. IT IS why I always say make them focused, conscious and MASSIVELY loving and intentional.
Reducing inflammation, living a #FullyOptimized lifestyle and having a spiritual (innerwork/mindful) practice are all huge keys in regrowing your hair. Adding in the adjuvants specifically discussed in part 2 next week will only makes things easier and compliment the other foundational principles.
What do you think of certain essential oils i.e. rosemary?
Quite effective in stimulating blood flow to hair follicles
Just literally rubbing a few drops in your hair daily? Also, how do you think hair products (fiber, pomade etc) affect the hair thinning?
Valid concern Mike.
I recommend you avoid Polyethylene Glycol which is frequently included in hair products including pomades.
To avoid hair breakage, be cautious about products that require you to shampoo your hair frequently as they dry your hair shaft (fibers).
As a woman who had hair loss I was prescribed spironolactone and Proscar in my late 20’s. My scalp hair regrew to be as thick as it was in high school, massive head of gorgeous hair. So the meds did work for me big time. It also reduced excess body hair on my body. Now I am 43 now and my hair started falling out bc of thyroid issues. Looking forward to hearing what this guy says works bc I haven’t seen anything else work for hair growth/loss.
I have always suspected lower GH and IGF-1 play a role as well.
Definitely. Hormonal Health is super critical
I am interested to see if Derek from More Plates More Dates will weigh in on his youtube channel. I suspect that he will agree that hair loss is caused by multiple factors, but that DHT is one of them, and that finasteride is generally the “go to” treatment for much of the population. My guess is that DHT is a factor, but that inflammation and circulation are also likely factors too. I don’t think the hair loss world is entirely wrong about DHT since finasteride seems to work for many people despite potential side effects.
Hair loss is also just a factor in aging. How many over the age of 80 have a full thick head of head? Maybe 1% or less?
On a related subject, some people anecdotally report that creatine causes hair loss for them, presumably due to it causing an increase in DHT.
It’s interesting to note that many foods that cause a decrease in DHT also seem to cause a decrease in cancer. For example, cruciferous vegetables, mushrooms, tomatoes. berries, avocadoes, carrots and nuts.
I suspect that DHT is probably neither good nor bad in itself, but likely needs to be at the right level for optimum hair and health.
Thanks for your comments Jack.
Hair loss is definitely a factor in aging but if one can stimulate active and healthy follicles by the multiple means described in Part 2 of the article(coming next week), there is no reason why reasonable regrowth isn’t achievable. We have thousands of customers that already prove this.
Both Nick and I would be happy to have a conversation with Derek about this topic. The science is sound and proven in this article and results are being further experienced by thousands of Men and Women across the world using Auxano Grow V2.
Inhibiting natural biological processes/pathways like Estrogen or DHT is not prudent for the long term health of the organism. Anything said to counter that is not born out by the scientific evidence nor the results experienced by a significant number of individual from many negative lifestyle measurements.
Jack thanks for sharing this.
It’s interesting that there are several comments mentioing creatine here. I recently observed that my hair was becoming noticeably thinner while my hairline was slightly receeding, as well as an increase in body hair where there was previously little/none hair present. I made a list of about 20 things that occurred or changed in the last four to six months that may have led to this. My top two suspects are 1) creatine supplementation and 2) daily photobiomodulation on entire body (yes, including testes). It could be either of these, the combination of these two variables, or something else entirely.
I would love to hear anyone else’s experience or thoughts on this, especially with regard to photobiomodulation and creatine.
My God, you look miserable in that photo.
Haha. Thanks, I think.
Yeah that photo is really strange on multiple levels.